A new paper is out that definitively concludes absolutely, without question that masks/respirators reduce transmission of respiratory infections.

It's important that this work is published, but it's a shame that it's so necessary ONLY because there are so many misinformed nay-sayers who objected to mask mandates enough to actually influence policy to the point that some Health Care workers don't even mask near infectious or immunocompromised people - even around preemies - because they don't have to anymore. It's important because Covid is still here, of course, still killing and disabling people daily, but also TB, measles, and whooping cough have made a huge comeback. I'm not sure this paper will change policy or public opinion, though. We're well immersed in post-truth governments at this point. But at least it's something I can wave around when people tell me I've been duped by lies from, um big-Covid?? And I really, really hope the paper makes an impact on our nose-diving culture.
Here's co-author Trisha Greenhalgh's salty thread on this incredible paper in full below. Loud letters are hers, but anything bolded is my emphasis:
"13 authors, 38,000 words. 413 references. One conclusion: these devices work.
The commissioned review, which was independently peer-reviewed, had 3 objectives: 1. Summarize the evidence on masks/masking. 2. Examine why this evidence is so widely misunderstood, misinterpreted, or dismissed. 3. Outline an agenda for future research. Author team was chosen for breadth of expertise, including: public health, epidemiology, infectious diseases, biosecurity, fluid dynamics, materials science, mathematical modeling, data science, clinical trials, sociology, anthropology, psychology, and occupational hygiene. Author team, which includes D.A. Lupton, D. Fisman, A. Kvalsvig, R. MacIntyre, S. Bhattach, J. Vipond, and others from Kirby Institute, M. Ungrin, M. Oliver, also had expertise in multiple kinds of evidence synthesis, including statistical meta-analysis. Study protocol for this narrative review with embedded meta-analysis was registered on INPLASY.
We searched extensively for high-quality evidence in all fields. We did NOT assume that all RCT evidence was “gold standard”, nor that all non-RCT evidence was “low-quality”. Indeed, we questioned whether the RCT deserves its hallowed status in this field.

We covered evidence across a vast range of disciplines and study designs, including but not limited to: laboratory studies, RCTs, observational studies, modelling studies, social and psychological studies, surveys, policy analyses, environmental impact studies. We went through the basic science showing that SARS-CoV-2, like other respiratory infections, is transmitted via the air. We criticised EPISTEMIC TRESPASSING by infection prevention and control (IPC) physicians, who drew wrong conclusions from their own flawed experiments.

We carefully traced the origins of the widely-propagated “droplet hypothesis”, in which it is assumed that large droplets somehow get deep into the lungs on some kind of ballistic trajectory (tip: they don’t).

Why does this matter? Because IF the droplet hypothesis were correct (TL;DR: it’s not), all we’d need is one of those baggy, waterproof-backed ‘medical masks’ designed to stop the surgeon sneezing into the patient’s open abdomen or getting a mouthful when an abscess bursts. But because respiratory infections transmit via TINY PARTICLES SUSPENDED IN THE AIR, waterproof-backed medical masks are NOT the best way to stop them. Starting from first principles, what we need is something that EFFICIENTLY REMOVES PARTICLES FROM THE AIR. In other words, not all things you put over your face are equal! Here’s a few things to think about:


Are you with me? There are good ways and bad ways of designing a mask! Ideally, you want one that's guaranteed HIGH-FILTRATION, LOW-RESISTANCE, WELL-FITTING and SUPER-CLEAN. Such a device is known as a RESPIRATOR. 2 examples shown: N95 (single-use) and elastomeric (reusable).


Did we address the anti-maskers’ favourite argument that the holes in a mask filter are bigger than the SARS-CoV-2 virus? What do you think? Of course we did. MASK FILTERS ARE NOT SIMPLE SIEVES!

Here’s a nice diagram. Each little square is a different laboratory study. ‘Filtering facepiece’ means RESPIRATOR. ‘Community mask’ means one you made at home (from cloth). ‘Protection factor’ (note: LOGARITHMIC scale) is how much it blocks bad particles (higher is good).

The above diagram is from Schmidt & Wang’s paper on the CRITICAL ROLE OF LEAKAGES in mask malfunction. If air leaks out around the sides = less protection. We thank these authors for letting us reproduce it. Another leakage study. Up the side is LEAKAGE (more is bad). Along the bottom is particle size. Different colours represent different masks: GREEN = medical mask (very leaky), PURPLE = respirator sealed all around with tape to get perfect fit (nothing gets through it).

OK, we’re getting to the RCT section. And this is where the quality of much of the evidence plummets—partly because there’s some flaky trials out there and partly because even the BEST trials of masks are INHERENTLY problematic.


Most RCTs of masks didn’t use an optimally-designed device. Many didn’t measure whether the mask was worn (where compliance was measured, was low). These flaws are like doing a RCT of a blood pressure drug at 1/100th the correct dose. They BIAS THE RESULT TOWARDS THE NULL. Other common flaws in mask RCTs include lack of power, suboptimal outcome measures, telling participants to only mask SOME of the time, and doing the study when there are no infections circulating. Each of these slip-ups will tend to bias results towards null. Small wonder, then, that most RCTs of masks in community or in healthcare settings produced no statistically significant difference between the ‘mask’ arm (actually, the “advice to slap a poorly-designed medical mask on if you feel inclined” arm) and the ‘no mask’ arm. The one adequately-powered RCT of community masking in the entire sample (which cluster-randomised villages in Bangladesh), by Abaluck et al, showed a statistically significant effect in favour of masks even though compliance was low.
Let’s talk about RCTs of masks v respirators in healthcare. The research question here is of the utmost importance. Should we protect our staff with the kind of device that produced the purple line in the graph above? Or should they get the device that produced the green (leaky) line? Here’s where the study designs go embarrassingly off. Because many IPC doctors falsely believe the droplet hypothesis, their prior belief (which influences the intervention design) is that medical masks are as good as anything else so long as you wash your hands. IPC docs may also believe that infectious aerosols are produced by a patient only when they’re having a fancy procedure done to them by a doctor (hence ‘aerosol-generating medical procedure’ AGMP). (You’re right, it does rather smack of infantile omnipotence) In fact, patients infected with SARS-CoV-2 (or SARS-1 or MERS or influenza or measles or TB) emit infectious particles in the air by COUGHING and SPEAKING and even BREATHING. And those particles quickly spread THROUGHOUT THE INDOOR SPACE. Hence, any trial of masks v respirators in a healthcare setting MUST require the devices to be worn CONTINUOUSLY WHEN INDOORS. If higher-grade protection is worn only when close to a known ‘case’ or when doing an AGMP, it’s likely to be as good as a chocolate teapot.
We meta-analysed mask-v-respirator trials in healthcare settings in two ways. First, lumping all trials together (result: respirators outperform masks a bit). Second, using only RCTs testing CONTINUOUS USE OF RESPIRATORS. Result: respirators outperform masks significantly. Acknowledging the limitations of observational evidence, we identified and summarised LOTS of observational studies and natural experiments. All studies pointed in the same direction: in favour of the kinds of effect you’d predict from basic science. Likewise with mathematical modelling studies (of which there are various kinds). In sum, the non-RCT evidence – rather surprisingly and very consistently – stacks up in favour of masks (and of respirators as even better).

HARMS of masks. Three kinds: 1. Complete fictions (things the anti-maskers make up, like accumulation of poisonous CO2 in your body—it doesn’t happen). 2. Minor hazards (headaches, acne), which may be worth the trade-off. 3. Specific exemption conditions

When OTHERS are masked, there may be communication problems, especially for D/deaf people. One of our authors, Amanda Kvalsvig, is hearing-impaired. She wrote: it MAY NOT be in a deaf person’s interests if others remove their masks! (It may, but need to WEIGH UP RISKS). We need better communication strategies that can be employed if mass masking needs to be introduced again. We talk about some avenues for this in the paper (e.g. lapel mics so we don’t tire out our voices). More research needed on these!
WHY DO PEOPLE MASK (and why do some REFUSE TO MASK)? Answer: for lots of psychological, cultural, ideological and social reasons, as D. Alupton says in her section.


Misleading messages from leading public health agencies contributed to confusion about masks and about the relative benefits of respirators versus medical masks.

Mask POLICIES involve strongly recommending and even mandating the wearing of masks in certain settings. We do a long section on this. Policymakers need to ASSESS THE RISKS, BALANCE THE TRADE-OFFS and SUPPORT THE POLICY (e.g. by giving them away). Single-use masks and respirators are not good for the planet. It’s time we moved to a more sustainable approach. Re-usable, recyclable and biodegradable devices exist. DID YOU KNOW that you can recycle chopped-up masks to make building materials like concrete?
Time for conclusions. First, MASKS WORK!!! And we’ve explained why some people insist that they don’t! Read the yellow bit out loud please.

Second conclusion. It’s time to REMOVE PEOPLE WHO CAN’T OR WON’T UNDERSTAND THE EVIDENCE ON MASKING FROM KEY DECISION-MAKING COMMITTEES. Who will be brave and make that move? Lives depend on it.

Third conclusion. Mask policies should be based on ACTUAL risks, not SPECULATIVE ones. And masks, overall, should be better designed to REDUCE the minor side effects like hot face.

Fourth conclusion. Talking of design, we need CREATIVE DESIGNS to suit EVERYONE, not just your standard crash-dummy white 70Kg clean-shaven male.

Fifth conclusion. Let’s make masks sustainable.

Final conclusion: anti-mask disinformation is as dangerous as anti-vax disinformation. We need to systematically counter it.

BOTTOM LINE: We don’t need any more masks-on v masks-off RCTs. That’s for dobbins. We need a NEW GENERATION of research which takes as its starting point the VAST EXISTING EVIDENCE BASE on the efficacy of masks and respirators. Then this:

And here’s the piece on my Departmental website And here's our piece for The Conversation - also just out (you can syndicate)."
ETA: A little from Prof Raywat Deonandan:
"Just gonna put this out there. The military never did any RCTs to prove that gas masks work in the battlefield. They relied on lab testing. That's because they could depend on near perfect user compliance. That's what RCTs for engineering interventions really measure: compliance."
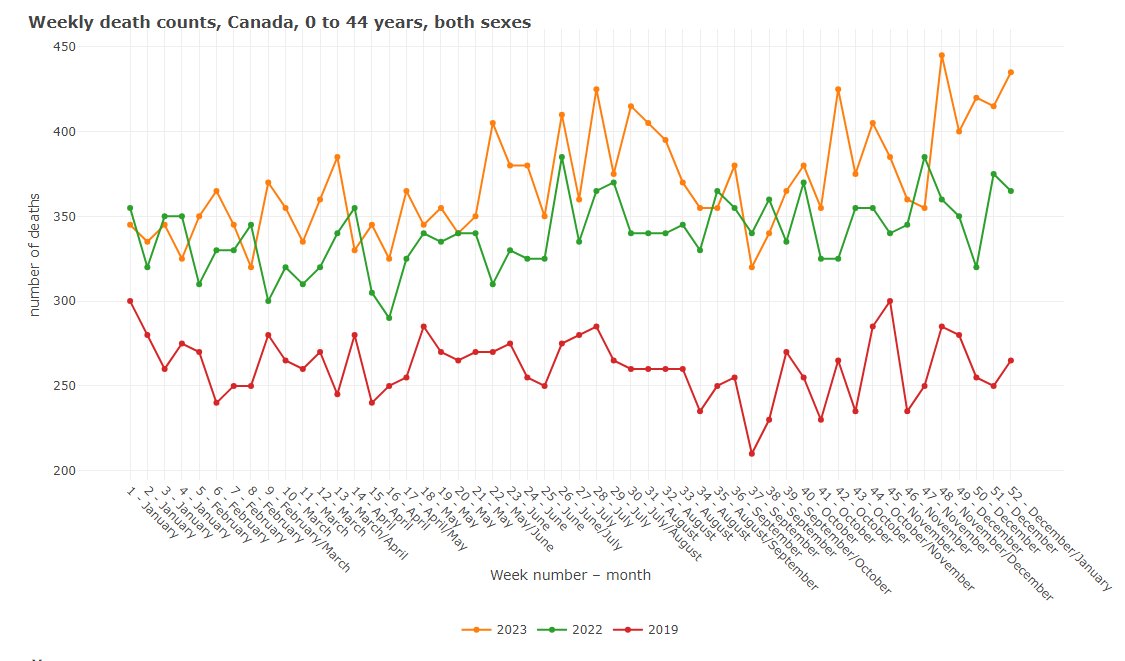
ETA, in case you think Covid is over or harmless, here's the excess death for Canadians 0-44 in 2019 (baseline in red), 2022 (green), and 2023 (yellow). In Ontario alone, we're looking at over 50,000 excess deaths last year.
2 comments:
Most would agree with these basic points. Most, though, would disagree with these conclusions.
SARS-Cov2 is airborne – true. I’m not sure why anyone thought otherwise.
Respirators reduce your chance of getting infected – true
The general public must do something to protect the vulnerable - no
Most people realize that COVID is not a significant threat. Whether we the original fear was overblown is irrelevant.
Society moves on.
The time for scientism that fails to value normal life has passed.
RE: The general public must do something to protect the vulnerable - no. Most people realize that COVID is not a significant threat." Covid is the third leading cause of death in Canada, second to cancer and heart disease, so if you do things to avoid those risks (exercise, quit smoking), you might want to do things to avoid Covid as well. We protect the vulnerable from cancer by making it illegal to smoke inside buildings, and it would make sense to clean the air of Covid too. Covid also leaves long term disabilities in its wake. Now that kids are dying of measles again, we need to step up protections for the vulnerable. Cleaning the air doesn't just help reduce Covid, but measles, TB, RSV, and the flu. Illnesses causing kids to miss school are far higher than pre-Covid. It's possible to avoid these viruses; I can't imagine why anyone would want them to continue.
Post a Comment